Incredible, Edible Robots
Incredible, Edible Robots

A tiny origami robot has unfolded after swallowing. External magnets direct it towards a wound in a stomach, where it can patch wounds, remove foreign objects, and examine obstructions. Photo: MIT
For as long as he can remember, David Zarrouk has loved to tinker and build things. Growing up, the director of Ben-Gurion University’s Bio-Inspired and Medical Robotics Laboratory used his pocket money to buy remote control cars and other electronic toys. He’d play with them for a little while—and then find ways to repurpose them. He was always looking for ways to revamp the design so they could better venture into difficult-to-reach places.
“I tried to build flying machines,” Zarrouk said. “Unsuccessfully, I should add. I even built a remote-control cheating machine that could drive notes out from under the desk during exams. I’ve always been interested in how to design robots for locations that are hard to get into and hard to move around in.”
He has pursued that interest throughout his career. From his undergraduate days through the founding of his own laboratory, Zarrouk has tried to design robots that can reach into some of the most hostile settings imaginable, such as collapsed buildings, flood zones, and radioactive waste sites.
In fact, he has made a name for himself creating robots with simple, elegant mechanics that can successfully traverse such demanding surroundings.
Now, he’s refining a robot that will have to navigate what may be the most inhospitable, hard-to-reach place of all: the human gastrointestinal (GI) tract.
Navigating the Interiors of the Body
According to the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), 60 million to 70 million people are affected by digestive diseases, ranging from ulcerative colitis to colorectal cancer.
According to Bincy Abraham, a gastroenterologist at Houston Methodist Hospital, it can be difficult for gut specialists like herself to diagnose many of those conditions because of the very nature of the digestive tract.
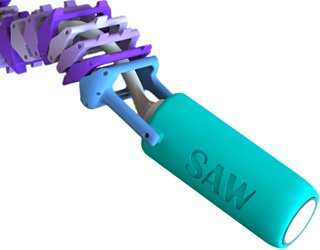 This single actuator wave (SAW) robot is slightly larger than a quarter and can crawl through slippery intestines. Image: Ben-Gurion University
“The GI tract is pretty long—about 30 feet long—and it twists and turns quite a bit,” she said. “And it’s an organ that is always secreting something. It’s full of gastric juices, pancreatic juices, bile acids, and waste. We use different tests and imaging methods to look for problems but, with such a complex organ, it can be difficult to find answers without surgery.”
This single actuator wave (SAW) robot is slightly larger than a quarter and can crawl through slippery intestines. Image: Ben-Gurion University
“The GI tract is pretty long—about 30 feet long—and it twists and turns quite a bit,” she said. “And it’s an organ that is always secreting something. It’s full of gastric juices, pancreatic juices, bile acids, and waste. We use different tests and imaging methods to look for problems but, with such a complex organ, it can be difficult to find answers without surgery.”
Of course, most gastroenterologists do not rush into surgery. Instead, they rely on an endoscope, a device made up of a flexible tube with a light and camera on one end. This lets them view the interiors of the body in a not-quite-as-invasive manner.
Read More About: Six Robots Helping Doctors Today
Yet endoscopes have serious limitations, Abraham explained. This starts with a significant risk of infection and injury. Often, they are not long enough to view the entirety of the GI tract. Nor are they always very maneuverable.
“There may also be strictures or narrowing of the intestines as you move through the tract,” she said. “So you may just have to go back the way you came and risk missing something.
“A solution that would allow us to get to the parts of the gut we need to see—to get a real-time image of what’s going on, to go back and recheck something, to zoom in or out on an area, to take a biopsy and store it in a compartment—that would be of great help to us and our patients.”
Robotic medical devices could provide an ideal answer to Abraham’s wish list, Zarrouk said. They could solve other physician requests, ranging from successfully dispensing medications or chemotherapy treatments to cauterizing wounds or surgically removing a diseased piece of tissue.
“We can design small robots to penetrate the body in minimally invasive procedures, reducing the danger to the patient and recovery time,” Zarrouk said. “This kind of approach can also help the doctor find potential problems and make these procedures more affordable. We just have to design it so it can get around in this very difficult place.”
Engineering an Edible Robot
Sending robots down the stomach and intestinal track sounds radical. Yet digital pills date back to 1957, when Bertil Jacobson of Karolinska Hospital in Stockholm invented a pill that could measure pressure waves as it moved through the small intestines.
Today’s pills are much smarter. In 2017, for example, Proteus Digital Health and Japanese pharmaceutical company Otsuka received Food and Drug Administration for an anti-psychotic drug, Abilify MyCite, that transmits information to a cellphone when a patient takes it.
In 2014, FDA approved the PillCam, an inch-long device with a video camera, lights, and a battery. Developed by Medtronic, it complements—and may one day replace—colonoscopies. Patients simply swallow the PillCam, and it transmits images as it naturally passes through the GI tract.
While Medtronic has improved this device over the past few years, it still cannot offer the kind of features that Abraham and other gastroenterologists would like. Robots might—and different labs across the globe, including Zarrouk’s, are working on devices that can offer enhanced capabilities and greater flexibility.
First, however, these researchers must solve some unique engineering challenges. The first one is size. Many people still struggle with swallowing even the smallest of vitamin pills. Asking them to down a thumb-sized robot is likely out of the question.
Daniela Rus, a professor of electrical engineering and computer science at the Massachusetts Institute of Technology, thinks she may have an answer: origami. Inspired by the ancient art of Japanese paper folding, she and her colleagues designed a small, ingestible robot that would be compact enough for patients to comfortably swallow yet unfold once in the body.
“The robot is made of two layers of dried pig intestine sandwiching a layer of biodegradable wrap that shrinks when it’s heated,” Rus said. “This allows it to be compressed like an accordion into an easy-to-swallow form.”
Once swallowed, the device pops open to its full size. Rus steers it by using magnetic fields. She thinks it she will be able to use the robot to catch a swallowed lithium battery, patch a wound, or deliver medicine.
 At Colorado University Boulder, researchers are developing an "endoculus" robot to replace endoscopes used for colonoscopies. The robot promises greater maneuverability and better images than existing technology. Photo: University of Colorado
“When the capsule dissolves, the forces acting on the robot have to be strong enough to make it fully unfold,” said Rus. “Through a lot of trial and error, we created a rectangular robot with accordion folds perpendicular to its long axis and pinched corners that act as points of traction. The robot can latch on to a button battery with its own magnet and then can be guided to the intestines so it can be excreted.”
At Colorado University Boulder, researchers are developing an "endoculus" robot to replace endoscopes used for colonoscopies. The robot promises greater maneuverability and better images than existing technology. Photo: University of Colorado
“When the capsule dissolves, the forces acting on the robot have to be strong enough to make it fully unfold,” said Rus. “Through a lot of trial and error, we created a rectangular robot with accordion folds perpendicular to its long axis and pinched corners that act as points of traction. The robot can latch on to a button battery with its own magnet and then can be guided to the intestines so it can be excreted.”
Of course, size is not the only issue. Gastroenterologists also want maneuverability. While Rus’s team uses magnets to move robots through the GI tract, other labs are taking aim at slippery intestinal tissue.
While PillCams rely on the body’s forces to propel them forward, doctors would like more control to move the robots where they want them to go.
“Robots can travel pretty well in a plastic pipe, but they don’t do so well in the intestine,” Zarrouk said. “Trying to get a robot to crawl in the intestine is like trying to drive a car in the mud; It can’t get traction and just gets stuck.”
Zarrouk has been working on the problem since his graduate student days.
While working on his doctorate, Zarrouk created a worm-like robot that gently clamped to the surface of intestinal tissue to move forward. It got stuck too often for Zarrouk’s liking, “dancing forward and backward without really moving anywhere.”
He thought wave locomotion would be an ideal solution, but he couldn’t come up with an elegant enough design that was small enough to work well in the GI environment. He put the notion aside. Then, a few years ago, he had an epiphany.
“I was teaching about springs in a mechanical design class,” he recalled. “It occurred to me that if you project a rotating helix, it’s practically an advancing wave. If you rotate a spring, the projection becomes an advancing wave. So I designed a robot—the single actuator wave-like, or SAW, robot—with a helix inside it that could produce this wave and have it move. And it moves quite well on this tissue.”
You May Also Like: Robotic Surgery Without the Robot
Others are trying to design materials that move easily on GI tissue without damaging it. Mark Rentschler, a professor of mechanical engineering at the University of Colorado at Boulder, is one.
“We figured out that by using micropatterned materials, or micropillars, on soft silicon material, we could get really good traction on the tissues,” Rentschler said. “These little features are so small that you can’t really see them. But you can feel them and they provide that traction without adhesion.”
Rentschler’s lab has used these materials to create both a robot with a segmented body that moves like an inchworm as well as one that resembles a small tank.
“The idea is that all sides of this robot are engaging with the tissue to move it along,” he said. “We use direct contact with the tissue for locomotion. We’re not using magnets, or swimming, or using the body’s forces. Those micropatterned materials give you that tread you need to engage with the tissue without having to use too much energy.”
Power is yet another design concern. Today’s PillCam has a battery life of about 12 hours. Yet sometimes, 12 hours is not enough time to travel the entire length of the human gut. How can robotics engineers design devices that can stay alive long enough to not only gather information but also accomplish tasks like biopsy, cauterization, or drug release?
Zarrouk’s team uses a single motor to help keep down energy costs.
“I believe good mechanics require simplicity,” Zarrouk said. “Having a single motor helps us to keep the robot small, but it also makes the robot more reliable. And it also helps us to make the robot very energy efficient.”
Giovanni Traverso, a gastroenterologist at Brigham and Women’s Hospital in Boston who works on ingestible drug delivery robots, uses the stomach’s own acid to power his devices.
“We took a lesson from an old high school textbook,” Traverso explained. “You can make a lemon battery using the acid inside the lemon to drive an electrochemical reaction between two metal electrodes. We recognized that stomach acid could also support that kind of reaction.”
Traverso and colleagues have now demonstrated that they can supply the energy needs of a drug release device for at least a week using stomach acid as their power source. It was just a matter of recognizing that the stomach can provide the chemicals necessary to transfer electrons in a galvanic cell, and then using that cell to power ingestible electronics.
“It’s not only the stomach than can do it,” he said. “We can even harvest energy from the intestines. So there’s a lot of potential here to find viable power sources that can help make these devices more of a reality.”
But what about control? Rus’s team uses magnets to guide their device. Zarrouk believes that remote control capabilities could be helpful.
Rentschler, however, believes ingestible robots might better serve patients if they are autonomous. He and his colleagues are taking a page from autonomous automobiles to provide ingestible devices the intelligence they need to get around the GI tract on their own.
“In some ways, it’s a simpler problem than autonomous cars,” Rentschler said. “We don’t have road signs, we don’t have pedestrians, we don’t have high speeds, and we don’t have a lot of unexpected things coming our way. What we do have is kind of a tunnel where you are, generally speaking, just going forward or backward. It allows us to do computation pretty well.”
Using just a single camera, they can measure speeds and positions that can then help guide the device as it navigates the colon.
“We’re basically trying to take all the knowledge from self-driving vehicles and then simplify it so we can do it quickly, in real-time, with a simple camera,” he said. “So far, it’s working out really, really well and raises the possibility that these kinds of devices can work without any kind of medical infrastructure.”
Moving toward Clinical Use
While all these labs are working on different engineering challenges, as well as different sets of healthcare requirements, they all see the benefits of a small and steerable robot that can replace current methods to investigate the human gut.
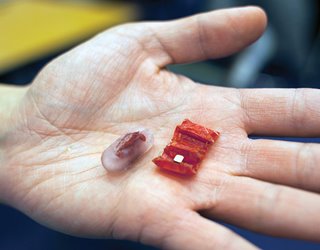 Patients swallow this ingestible robot in a pill. Once the pill dissolves, the robot unfolds and uses stomach acid to create a voltaic battery that powers its operations. Photo: Felice Frankel, MIT
Kyle Berean, a postdoctoral researcher in electronics and telecommunications engineering at Australia’s Royal Melbourne Institute of Technology who helped develop a pill sensor that measures gas levels in the digestive tract, says he believes that we are seeing the beginnings of a whole new field of robotic inventions in this space.
Patients swallow this ingestible robot in a pill. Once the pill dissolves, the robot unfolds and uses stomach acid to create a voltaic battery that powers its operations. Photo: Felice Frankel, MIT
Kyle Berean, a postdoctoral researcher in electronics and telecommunications engineering at Australia’s Royal Melbourne Institute of Technology who helped develop a pill sensor that measures gas levels in the digestive tract, says he believes that we are seeing the beginnings of a whole new field of robotic inventions in this space.
“Actually gaining access to what’s going on in the GI system—we’ve never had good access to that before,” he said. “What we’ve started is fairly simple, but it offers the possibility to do so much more in the future.
“Once we verify these devices’ clinical relevance, and get them into the hands of researchers and clinicians, we have the possibility of helping all those people, estimated to be about one in five in Western countries, who are suffering from gastrointestinal issues.”
Recommended for you: Mini Kidney on a 3D-Printed Chip
Zarrouk, meanwhile, continues to be excited by the possibility of designing medical devices that can go, to paraphrase that famous line from Star Trek: Where no medical device has gone before. With proper funding, he believes that we will see robots like his SAW in clinical use within the next five years.
“For more than 10 years, I’ve been searching for a solution for how to get a robot to move in this environment,” he said. “It’s been such an interesting problem to try to solve.
“Now that we are closer, there is the possibility that we can really make a difference in care. If we can meet these different challenges and create robots that can help treat patients in a better way—and maybe even save lives—it’s a big success from my point of view.”
Kayt Sukel is a science and technology writer based outside Houston, Texas.
“I tried to build flying machines,” Zarrouk said. “Unsuccessfully, I should add. I even built a remote-control cheating machine that could drive notes out from under the desk during exams. I’ve always been interested in how to design robots for locations that are hard to get into and hard to move around in.”
He has pursued that interest throughout his career. From his undergraduate days through the founding of his own laboratory, Zarrouk has tried to design robots that can reach into some of the most hostile settings imaginable, such as collapsed buildings, flood zones, and radioactive waste sites.
In fact, he has made a name for himself creating robots with simple, elegant mechanics that can successfully traverse such demanding surroundings.
Now, he’s refining a robot that will have to navigate what may be the most inhospitable, hard-to-reach place of all: the human gastrointestinal (GI) tract.
Navigating the Interiors of the Body
According to the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), 60 million to 70 million people are affected by digestive diseases, ranging from ulcerative colitis to colorectal cancer.
According to Bincy Abraham, a gastroenterologist at Houston Methodist Hospital, it can be difficult for gut specialists like herself to diagnose many of those conditions because of the very nature of the digestive tract.
This single actuator wave (SAW) robot is slightly larger than a quarter and can crawl through slippery intestines. Image: Ben-Gurion University
Of course, most gastroenterologists do not rush into surgery. Instead, they rely on an endoscope, a device made up of a flexible tube with a light and camera on one end. This lets them view the interiors of the body in a not-quite-as-invasive manner.
Read More About: Six Robots Helping Doctors Today
Yet endoscopes have serious limitations, Abraham explained. This starts with a significant risk of infection and injury. Often, they are not long enough to view the entirety of the GI tract. Nor are they always very maneuverable.
“There may also be strictures or narrowing of the intestines as you move through the tract,” she said. “So you may just have to go back the way you came and risk missing something.
“A solution that would allow us to get to the parts of the gut we need to see—to get a real-time image of what’s going on, to go back and recheck something, to zoom in or out on an area, to take a biopsy and store it in a compartment—that would be of great help to us and our patients.”
Robotic medical devices could provide an ideal answer to Abraham’s wish list, Zarrouk said. They could solve other physician requests, ranging from successfully dispensing medications or chemotherapy treatments to cauterizing wounds or surgically removing a diseased piece of tissue.
“We can design small robots to penetrate the body in minimally invasive procedures, reducing the danger to the patient and recovery time,” Zarrouk said. “This kind of approach can also help the doctor find potential problems and make these procedures more affordable. We just have to design it so it can get around in this very difficult place.”
Engineering an Edible Robot
Sending robots down the stomach and intestinal track sounds radical. Yet digital pills date back to 1957, when Bertil Jacobson of Karolinska Hospital in Stockholm invented a pill that could measure pressure waves as it moved through the small intestines.
Today’s pills are much smarter. In 2017, for example, Proteus Digital Health and Japanese pharmaceutical company Otsuka received Food and Drug Administration for an anti-psychotic drug, Abilify MyCite, that transmits information to a cellphone when a patient takes it.
In 2014, FDA approved the PillCam, an inch-long device with a video camera, lights, and a battery. Developed by Medtronic, it complements—and may one day replace—colonoscopies. Patients simply swallow the PillCam, and it transmits images as it naturally passes through the GI tract.
While Medtronic has improved this device over the past few years, it still cannot offer the kind of features that Abraham and other gastroenterologists would like. Robots might—and different labs across the globe, including Zarrouk’s, are working on devices that can offer enhanced capabilities and greater flexibility.
First, however, these researchers must solve some unique engineering challenges. The first one is size. Many people still struggle with swallowing even the smallest of vitamin pills. Asking them to down a thumb-sized robot is likely out of the question.
Daniela Rus, a professor of electrical engineering and computer science at the Massachusetts Institute of Technology, thinks she may have an answer: origami. Inspired by the ancient art of Japanese paper folding, she and her colleagues designed a small, ingestible robot that would be compact enough for patients to comfortably swallow yet unfold once in the body.
“The robot is made of two layers of dried pig intestine sandwiching a layer of biodegradable wrap that shrinks when it’s heated,” Rus said. “This allows it to be compressed like an accordion into an easy-to-swallow form.”
Once swallowed, the device pops open to its full size. Rus steers it by using magnetic fields. She thinks it she will be able to use the robot to catch a swallowed lithium battery, patch a wound, or deliver medicine.
At Colorado University Boulder, researchers are developing an "endoculus" robot to replace endoscopes used for colonoscopies. The robot promises greater maneuverability and better images than existing technology. Photo: University of Colorado
Of course, size is not the only issue. Gastroenterologists also want maneuverability. While Rus’s team uses magnets to move robots through the GI tract, other labs are taking aim at slippery intestinal tissue.
While PillCams rely on the body’s forces to propel them forward, doctors would like more control to move the robots where they want them to go.
“Robots can travel pretty well in a plastic pipe, but they don’t do so well in the intestine,” Zarrouk said. “Trying to get a robot to crawl in the intestine is like trying to drive a car in the mud; It can’t get traction and just gets stuck.”
Zarrouk has been working on the problem since his graduate student days.
While working on his doctorate, Zarrouk created a worm-like robot that gently clamped to the surface of intestinal tissue to move forward. It got stuck too often for Zarrouk’s liking, “dancing forward and backward without really moving anywhere.”
He thought wave locomotion would be an ideal solution, but he couldn’t come up with an elegant enough design that was small enough to work well in the GI environment. He put the notion aside. Then, a few years ago, he had an epiphany.
“I was teaching about springs in a mechanical design class,” he recalled. “It occurred to me that if you project a rotating helix, it’s practically an advancing wave. If you rotate a spring, the projection becomes an advancing wave. So I designed a robot—the single actuator wave-like, or SAW, robot—with a helix inside it that could produce this wave and have it move. And it moves quite well on this tissue.”
You May Also Like: Robotic Surgery Without the Robot
Others are trying to design materials that move easily on GI tissue without damaging it. Mark Rentschler, a professor of mechanical engineering at the University of Colorado at Boulder, is one.
“We figured out that by using micropatterned materials, or micropillars, on soft silicon material, we could get really good traction on the tissues,” Rentschler said. “These little features are so small that you can’t really see them. But you can feel them and they provide that traction without adhesion.”
Rentschler’s lab has used these materials to create both a robot with a segmented body that moves like an inchworm as well as one that resembles a small tank.
“The idea is that all sides of this robot are engaging with the tissue to move it along,” he said. “We use direct contact with the tissue for locomotion. We’re not using magnets, or swimming, or using the body’s forces. Those micropatterned materials give you that tread you need to engage with the tissue without having to use too much energy.”
Power is yet another design concern. Today’s PillCam has a battery life of about 12 hours. Yet sometimes, 12 hours is not enough time to travel the entire length of the human gut. How can robotics engineers design devices that can stay alive long enough to not only gather information but also accomplish tasks like biopsy, cauterization, or drug release?
Zarrouk’s team uses a single motor to help keep down energy costs.
“I believe good mechanics require simplicity,” Zarrouk said. “Having a single motor helps us to keep the robot small, but it also makes the robot more reliable. And it also helps us to make the robot very energy efficient.”
Giovanni Traverso, a gastroenterologist at Brigham and Women’s Hospital in Boston who works on ingestible drug delivery robots, uses the stomach’s own acid to power his devices.
“We took a lesson from an old high school textbook,” Traverso explained. “You can make a lemon battery using the acid inside the lemon to drive an electrochemical reaction between two metal electrodes. We recognized that stomach acid could also support that kind of reaction.”
Traverso and colleagues have now demonstrated that they can supply the energy needs of a drug release device for at least a week using stomach acid as their power source. It was just a matter of recognizing that the stomach can provide the chemicals necessary to transfer electrons in a galvanic cell, and then using that cell to power ingestible electronics.
“It’s not only the stomach than can do it,” he said. “We can even harvest energy from the intestines. So there’s a lot of potential here to find viable power sources that can help make these devices more of a reality.”
But what about control? Rus’s team uses magnets to guide their device. Zarrouk believes that remote control capabilities could be helpful.
Rentschler, however, believes ingestible robots might better serve patients if they are autonomous. He and his colleagues are taking a page from autonomous automobiles to provide ingestible devices the intelligence they need to get around the GI tract on their own.
“In some ways, it’s a simpler problem than autonomous cars,” Rentschler said. “We don’t have road signs, we don’t have pedestrians, we don’t have high speeds, and we don’t have a lot of unexpected things coming our way. What we do have is kind of a tunnel where you are, generally speaking, just going forward or backward. It allows us to do computation pretty well.”
Using just a single camera, they can measure speeds and positions that can then help guide the device as it navigates the colon.
“We’re basically trying to take all the knowledge from self-driving vehicles and then simplify it so we can do it quickly, in real-time, with a simple camera,” he said. “So far, it’s working out really, really well and raises the possibility that these kinds of devices can work without any kind of medical infrastructure.”
Moving toward Clinical Use
While all these labs are working on different engineering challenges, as well as different sets of healthcare requirements, they all see the benefits of a small and steerable robot that can replace current methods to investigate the human gut.
Patients swallow this ingestible robot in a pill. Once the pill dissolves, the robot unfolds and uses stomach acid to create a voltaic battery that powers its operations. Photo: Felice Frankel, MIT
“Actually gaining access to what’s going on in the GI system—we’ve never had good access to that before,” he said. “What we’ve started is fairly simple, but it offers the possibility to do so much more in the future.
“Once we verify these devices’ clinical relevance, and get them into the hands of researchers and clinicians, we have the possibility of helping all those people, estimated to be about one in five in Western countries, who are suffering from gastrointestinal issues.”
Recommended for you: Mini Kidney on a 3D-Printed Chip
Zarrouk, meanwhile, continues to be excited by the possibility of designing medical devices that can go, to paraphrase that famous line from Star Trek: Where no medical device has gone before. With proper funding, he believes that we will see robots like his SAW in clinical use within the next five years.
“For more than 10 years, I’ve been searching for a solution for how to get a robot to move in this environment,” he said. “It’s been such an interesting problem to try to solve.
“Now that we are closer, there is the possibility that we can really make a difference in care. If we can meet these different challenges and create robots that can help treat patients in a better way—and maybe even save lives—it’s a big success from my point of view.”
Kayt Sukel is a science and technology writer based outside Houston, Texas.
A tiny origami robot has unfolded after swallowing. External magnets direct it towards a wound in a stomach, where it can patch wounds, remove foreign objects, and examine obstructions. Photo: MIT

Freelance writer, author, and ghostwriter
Related Content

Jul 13, 2026
Exoskeleton Improves Mobility for Stroke Survivors

University of Utah researchers are piloting a 5.5-pound wearable robotic solution to help individuals with hemiparesis walk.

Jun 22, 2026
Blaze-Battling Bots Ahead

A novel system that uses AI-powered robots to extinguish fires could eliminate the need to put firefighters in dangerous situations.

May 21, 2026
Touchless Movement Through Fluidic Torque
Fluid-generated torque generated by microrobot swarms can move passive objects in surprising ways—without the need for physical contact.

May 19, 2026
Soft Robots Made Fast and Cheap

A new ultra-low-cost fabrication method makes soft robots faster and cheaper to build, opening the field to wider use in research and education.